Appearance
Clinical Documentation
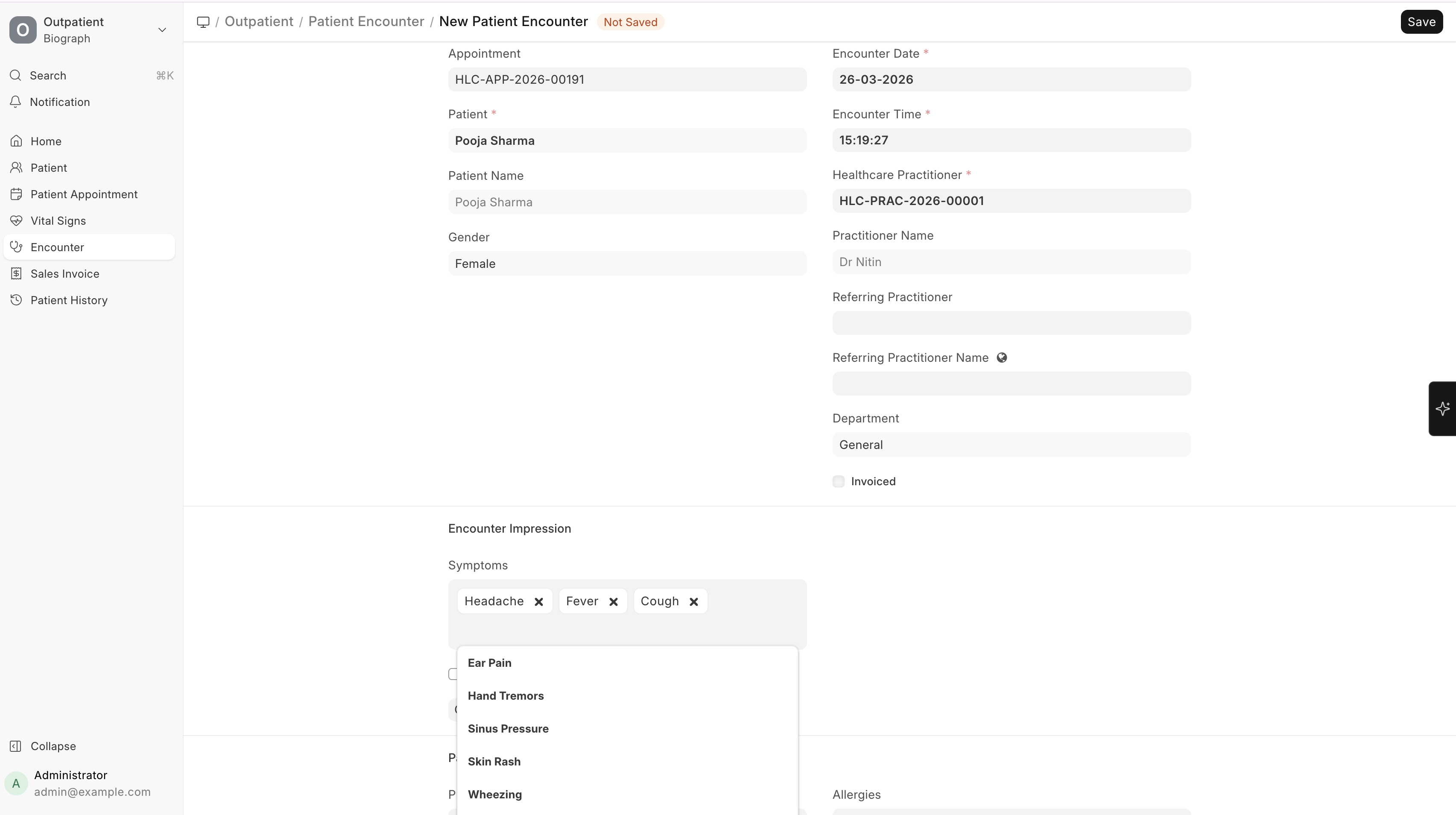
Complaints (Symptoms)
Record what the patient reports:
| Field | Description |
|---|---|
| Complaint | Select from master list or type a new one (e.g., Fever, Headache, Cough) |
| Duration | How long the patient has had the symptom |
| Severity | Mild, Moderate, Severe |
| Notes | Additional details about the complaint |
Tip: Frequently used complaints can be pre-configured in the Complaint master for quick selection via dropdown.
Diagnosis
Record the practitioner's clinical assessment:
| Field | Description |
|---|---|
| Diagnosis | Select or enter the diagnosis |
| Medical Code | Linked ICD-10 or SNOMED code (for standardized reporting) |
| Description | Additional notes about the diagnosis |
Multiple diagnoses can be recorded per encounter (primary and secondary).
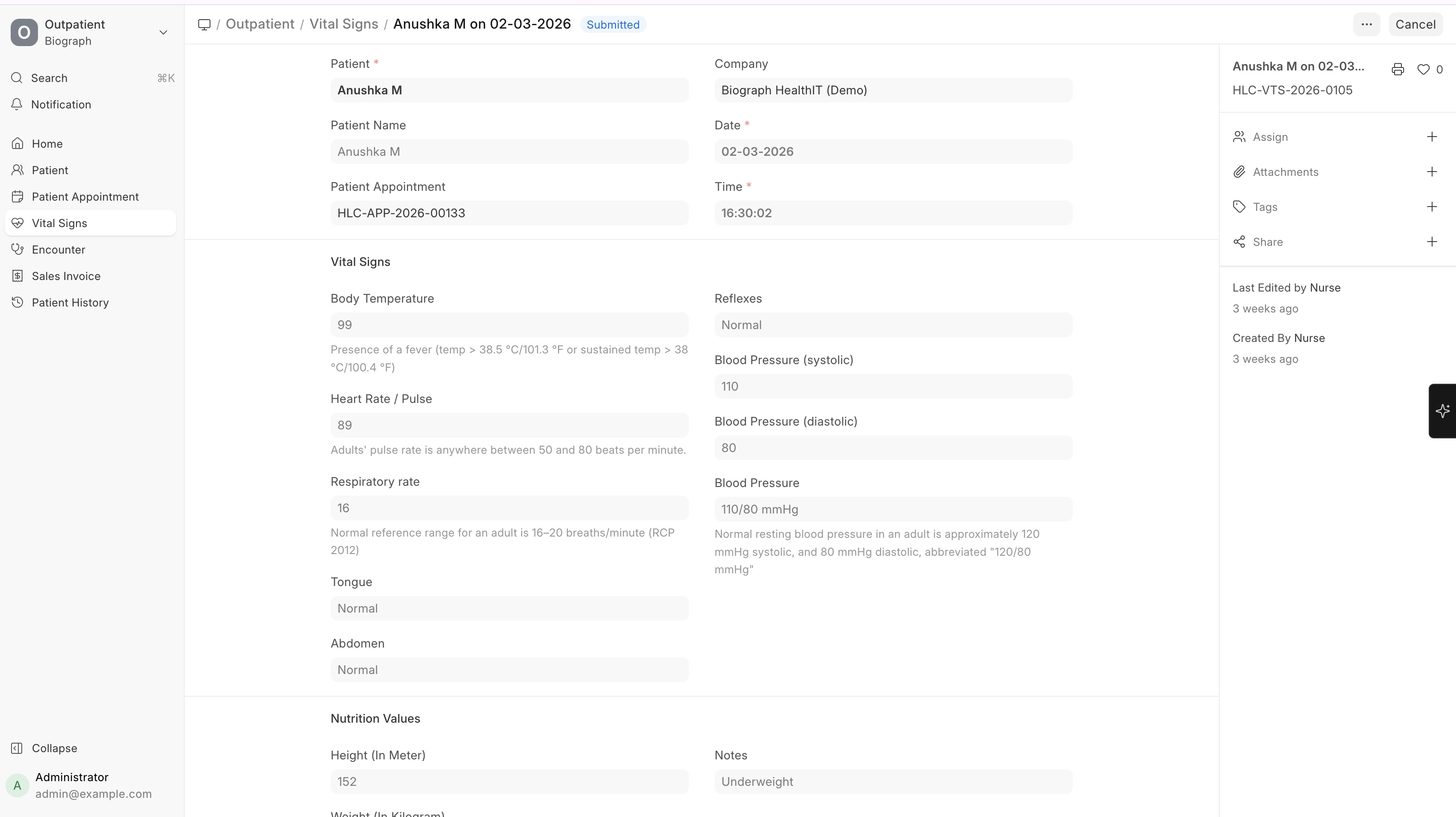
Vital Signs
Vital signs can be recorded directly within the encounter or via a separate Vital Signs record:
| Vital | Unit |
|---|---|
| Temperature | °F or °C |
| Pulse / Heart Rate | bpm |
| Respiratory Rate | breaths/min |
| Blood Pressure | mmHg (systolic/diastolic) |
| SpO2 | % |
| Height | cm |
| Weight | kg |
| BMI | Auto-calculated from height and weight |
| Nutrition Notes | Dietary observations |
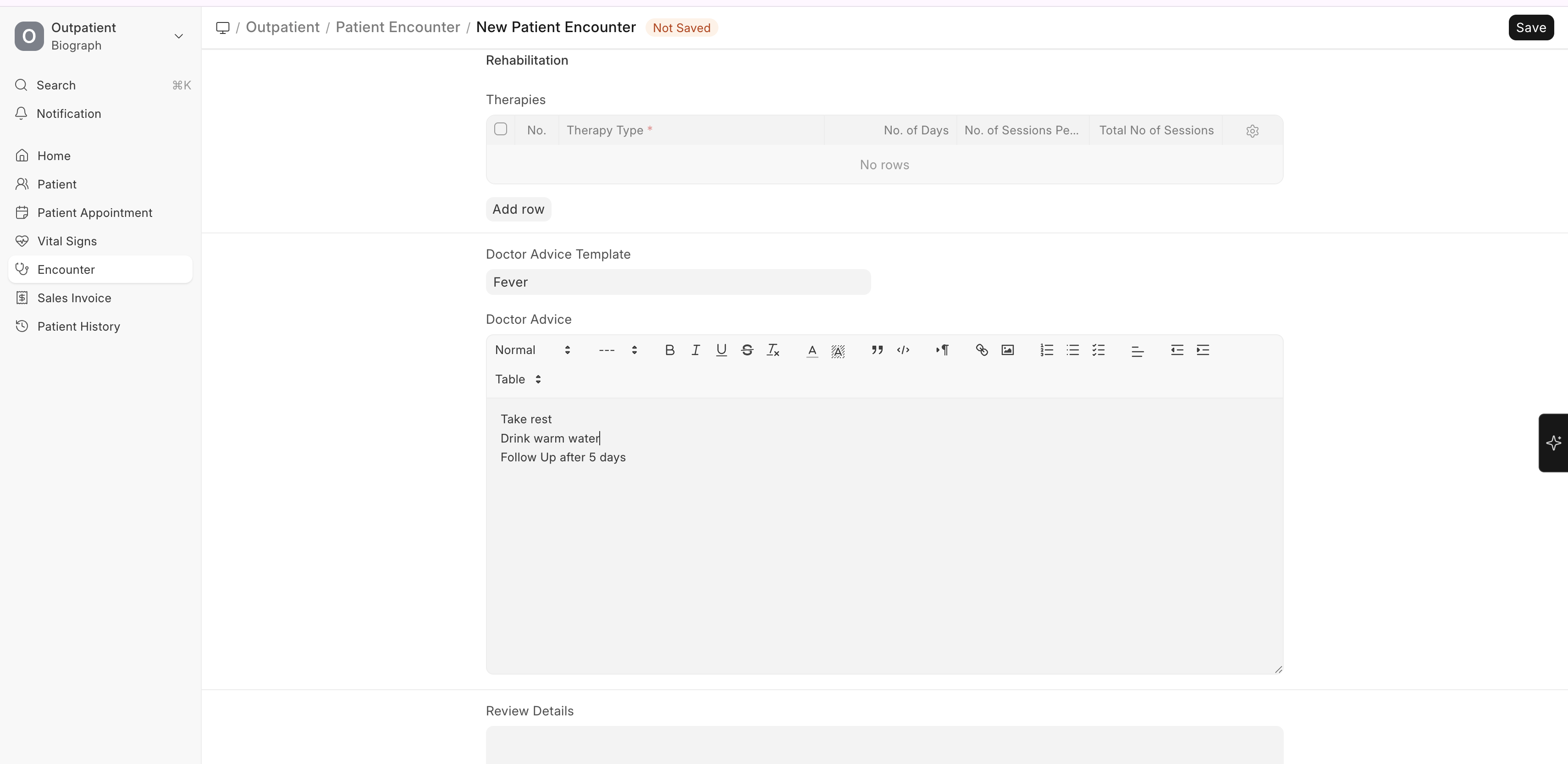
Clinical Notes
Free-text areas for comprehensive documentation:
- Examination details — Physical examination findings
- Clinical notes — Practitioner's observations and assessment
- Doctor Advice — Instructions given to the patient
Doctor Advice Templates can be pre-configured for frequently given advice (e.g., "Rest for 3 days", "Avoid spicy food", "Return if symptoms worsen").